Posture, etiology of a syndromePaolo
Platania
|
Posturology
guidelines and
interdisciplinary case study |
||||||
|
|
|
|
Posturology
|
The case study
|
The backstage
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Etiopathogenesis
This section presents the etiological hypothesis to both components of platania's syndrome:- Hypoglossal Nerve Neuropathy (HNN): as first primary etiopathogenesis of either Tongue motor insufficiency (TMI) and Dental Conflict (DC) pathomechanics,
- Pharyngeal Afferences Disorder (PAD): although uncovered by the rest of the case study, this hypothesis is under investigation as possible concurrent first primary etiopathogenesis of Tongue motor insufficiency (TMI),
- Maxillary Arch Insufficiency: as second primary etiopathogenesis of Dental Conflict (DC) only.
Inheritability: the presence of Maxillary Arch Insufficiency in patient's mother, affecting left emiarch as well, suggests inheritability and predisposition;
Congenit origin: the following symptoms and indicators are present since early childhood and are ascribable to Tongue Motor Insufficiency (TMI) or Dental Conflict (DC) pathomechanics
- deciduous teeth extractions due to development disorder suggests early presence of Maxillary Arch Insufficiency;
- first oral orthotics (failed attempt) appliance at age 6 due to teeth development disorder suggests early presence of Maxillary Arch Insufficiency as well;
- first memories of left side motor disorder (Head Forwarding Postural Strategy (HFPS)) are dated age 17 and may be described as easiness in stumbling on the left stride;
- ingrown toe nails on the left foot since age 7 witness the left side motor disorder (Ese01).
| ETIOPATHOGENESIS: Hypoglossal Nerve Neuropathy (HNN) (first primary) | |||||||||||||||
|
Hypoglossal Nerve Neuropathy (HNN) is the term to generally describe the neurogenic origin of tongue weakness , its exact diagnosis is hereby theorized. The evidences collected reasonably entitle Tongue Motor Insufficiency (TMI) as pathogenetic factor of Platania's Syndrome, this section gathers clues of its neurogenic origin (Ecl20 and Ese08), of lesion localization (Ethn01, Ethn03) and of broad diffusion of the same lesion in the population (Ethn02). |
|||||||||||||||
| # | Description | ||||||||||||||
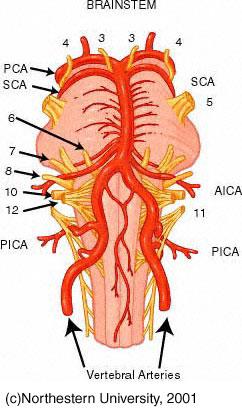
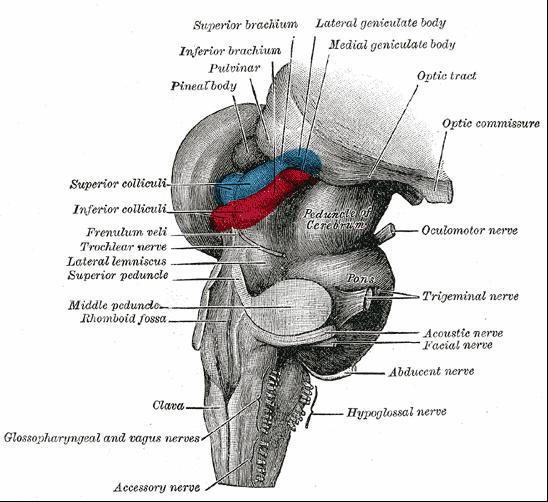
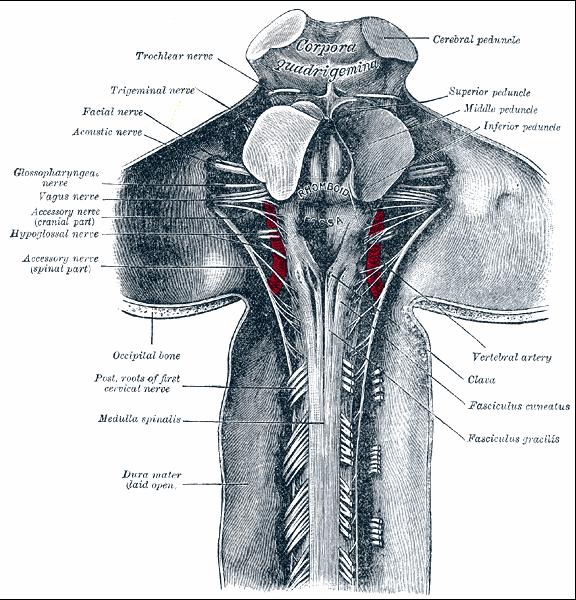
| Ethn01 | Hypoglossal Rootlets Emergence Entrapment (HREE) (This hypothesis is currently submitted to validation protocol (STAGE 4) to get more precise and instrumental clues.) Clue of HREE in the patient MRI (Ddo09).  click to enlarge Intracranial neurovascular conflict: Hypoglossal Nerve (HN) / Vertebral Artery (VA) conflict seems to be a recurrent condition [19]. Hypoglossal rootlets, at their emergence from medulla oblongata, often appear crossed, entrapped and compressed by a branch of Vertebral Artery (VA). The likelyhood of conflict between Hypoglossal Nerve (HN) and Vertebral Artery (VA) is enforced by their anatomical shape and relationship:
Below are presented some samples of conflictual HN/VA relationship and some anatomical higlights, the collection is a random selection of images returned by google internet search engine (with keywords like "vertebral artery", "medulla oblongata", "brainstem") and witness that this neurovascular conflict is as diffused as overlooked. |
||||||||||||||
|
|||||||||||||||
|
Although no literature ascribes neurogenic symptoms to this recurrent finding, it's opionon of the author that such an apparently asymptomatic neurovascular lesion may instead yield a sufficient amount of tongue weakness to provoke the reaction described in Platania's syndrome, together with vertebro-basilar vascular insufficiency and vessel sufferance and their higly harmful potential. Given the relevance of this hypothesis to Platania's syndrome, for easyness of reference this neurovascular conflict lesion is hereby baptized Hypoglossal Rootlets Emergence Entrapment (HREE). |
|||||||||||||||
| Ethn02 | HREE Diffusion in the population |
||||||||||||||
| Ethn03 | Other neurogenic etiologies (The following etiopathogenetical option are not under current investigation)
Anatomic variations inducing lesion: whatever vein / artery / vertebra / gland (parotid). Lower motor neuron disease Upper motor neuron Neuromuscular surgical complications Post surgical aberrant innervation [9] after childhood's tonsillectomy Other surgical complications |
||||||||||||||


| ETIOPATHOGENESIS: Pharyngeal Afferences Disorder (PAD) (first primary) | |||||||||
|
This hypothesis may concur in Cranio-Cervical Extension (CCE),
although may not explain Tongue Motor
Insufficiency (TMI), it deserves full consideration because it is wise
to exclude its partial involvement in the etiopathogenesis.
Pharyngeal Afferences Disorder (PAD) may explain AUCCE but not PUCCE and SBCCE, furthermore, regression events may be ascribed to temporary pharyngeal mucosa sensory loss due to contextual factors. |
|||||||||
| # | Description | ||||||||
| Etph01 | Pharyngeal over sensitivity (Although untreated by the rest of the case study, this hypothesis requires to be explicitly excluded) This condition may be induced by vagal nerve over sensitivity or pharyngeal airflow receptors exaggerated afferent signal and may mimic airflow insufficiency to central nervous system, thus eliciting Upper Airway Patency Maintenance Reflex (UAPMR) to induce AUCCE. |
||||||||
| ETIOPATHOGENESIS: Maxillary Arch Insufficiency (MAI) (second primary) | |
| To be completed | |
| # | Description |
| Etmi01 | To be completed |
|
Bugs report and technical issues notification to the webmaster are highly apreciated
|
| Posture, etiology of a syndrome - ©2008 Paolo Platania |